Any patient with gross hematuria or significant microscopic hematuria should have further evaluation of the urinary tract. The first step is a careful history and physical examination. Laboratory analysis consists of a urinalysis and examination of urinary sediment under a microscope. The urine should be evaluated for protein (a sign of kidney disease) and evidence of urinary tract infection. The number of red blood cells per high-powered field should be determined. In addition the shape of the blood cells should be evaluated. This can help determine where the bleeding is coming from. In patients with white blood cells in the urine, a urine culture should be performed as well. A urinary cytology is also obtained to look for abnormal cells in the urine. A blood test should also be done to measure serum creatinine (a measure of kidney function). Those patients with significant protein in their urine, abnormally shaped red blood cells, or an elevated creatinine level should undergo general medical evaluation for the presence of kidney disease.
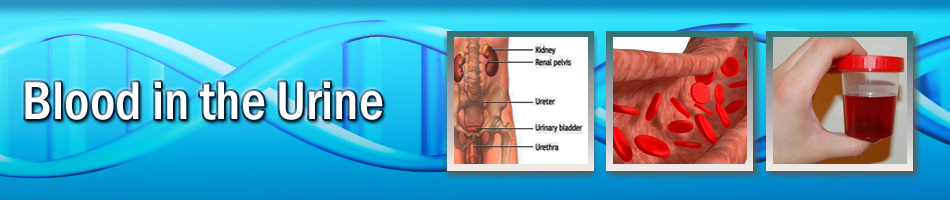
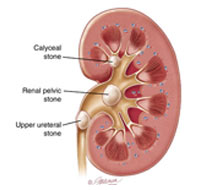
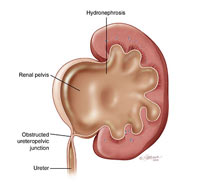
A complete urologic evaluation for hematuria also includes X-rays of the kidneys and ureters to detect kidney masses, tumors of the ureters and the presence of urinary stones. This traditionally consisted of an intravenous pyelogram (IVP). In this study, a radiographic dye is injected into the blood stream and X-rays are taken as the kidneys excrete the dye. This study has trouble detecting small renal masses and is often combined with a renal ultrasound.
Many physicians may opt for other imaging studies such as a computerized tomography (CT) scan. This is the preferred method of evaluating kidney masses and is the best modality for the evaluation of urinary stones. Recently many urologists have been using CT urography. This allows the urologist to look at the kidneys and ureters with one X-ray test. In patients with an elevated creatinine or an allergy to X-ray dye, magnetic resonance imaging (MRI) or retrograde pyelography is used to evaluate the upper urinary tract. During retrograde pyelography, the patient is taken to the operating room and dye is injected up the ureters from the bladder and then images are taken.
The main limitation of these imaging studies is the inability to evaluate the bladder; therefore a cystoscopic evaluation is required. This is usually performed in the office under local anesthesia with either a rigid, or more commonly, a flexible cystoscope. After applying a topical analgesic to the urethra the urologist inserts an instrument called a cystoscope through the urethra and into the bladder. Looking through the cystoscope the doctor can examine the inner lining of the bladder and urethra for abnormalities.
|